







NEUROPAIN develops physiological, pre-clinical and clinical research on pain. It develops its research working
almost exclusively on human beings
The group is committed with three main research axes:
- the study of cortical mechanisms leading to, and modulating pain perception in humans (Pain Physiology);
- the use of neurophysiological techniques to improve our understanding, diagnosis and prediction of neuropathic pain (PathoPhysiology of Pain);
- the improvement of cortical neurostimulation procedures for pain relief through a better comprehension of their mechanisms (NeuroStimulation).
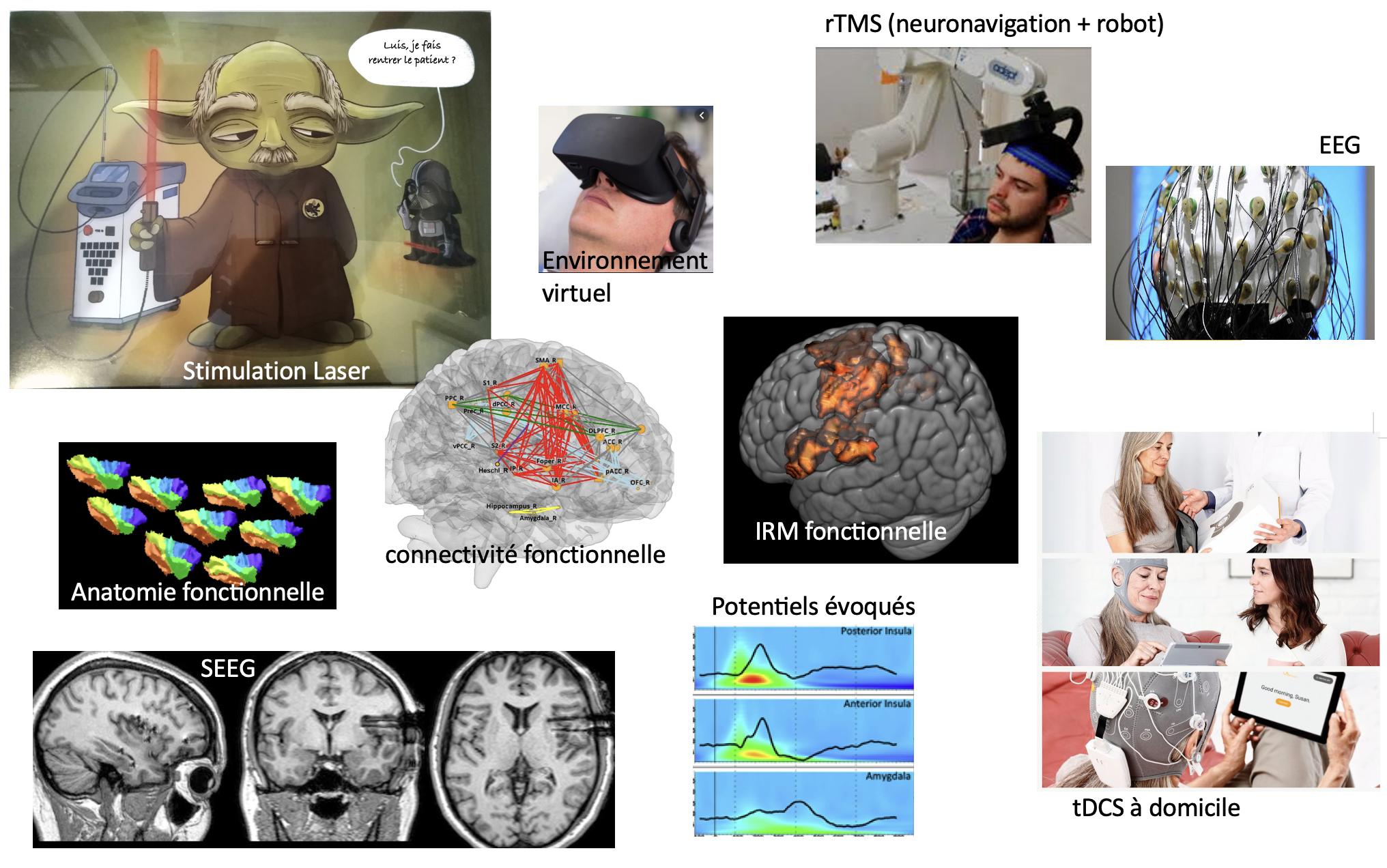
The team is physically located within the Neurological Hospital of Lyon and the University hospital of Saint-Etienne. Most of the team members have clinical activities, hence ensuring direct access to clinical facilities and patient wards. NeuroPain has dedicated systems for high-density electrophysiology (2x128- channel EEG) and cortical stimulation (rTMS, tDCS, epidural and intracortical stimulation), as well as 3D neuronavigation facilities with robotized arm and several multi-modal sensory stimulation systems, including two nociceptive-specific Nd:YAP laser stimulators. We have access to MEG, fMRI and PET- scan facilities, as well as to the platform for intracranial EEG, which is coordinated by one of our team members. NeuroPain is also founding member of, and directly involved in the development of the platform “Neuro-Immersion”, coupling Virtual Reality with HD-EEG, TMS and 3-D real-time kinematics.
NeuroPain joins efforts of 20 tenured members: neurobiologists, neurologists, psychologists, neurosurgeons, research engineers.

2 researchers INSERM or University St-Etienne
- 3 technical / ingeneer support staff
- 13 clinicians
Psychophysics, EEG, intracranial EEG, anatomical and functional MRI, PET, neuronavigated rTMS, tDCS
Signal and image processing, brain oscillations, source modeling, connectivity.
Physiology and Pain Modulation
• Spatiotemporal Analysis of Pain Information Processing
- Understanding the Cortical Determinants of Subjective Pain Perception
(M. Frot, M. Guenot, H. Bastuji)
- Analysis of Intracerebral Functional Interactions Related to Pain Perception
(C. Fauchon, L. Modernell, I. Faillenot)
• Interaction with Attentional and Emotional Cognitive Mechanisms
- Cortical Integration of Painful Emotional Faces
(M. Frot)
- Decoding Pain Signals in an Auditory Stimulus: A Baby's Cry
(S. Corvin, C. Fauchon, I. Faillenot, R. Peyron, Coll. N. Mathevon, ENES)
• Pain Memory
(M. Frot, C. Perchet)
- Pain Memory Related to a Context
- Memory of the Context Associated with the Pain
Diagnosis, prevention, and characterization of neuropathic pain
• European project on the detection of pain biomarkers
(L. Garcia-Larrea)
• Laser Evoked Potentials in clinical practice for the diagnosis of neuropathic pain
(L. Garcia-Larrea, C. Perchet)
Non-pharmacological treatments for chronic pain
• Study of rTMS and tDCS for pain relief
- Follow-up of a cohort of patients treated with rTMS and then with cortical electrodes
(R. Peyron, J. Thomas, C. Quesada, L. Garcia-Larrea, F. Vassal)
- Transcranial electrical stimulation (tDCS) program at home (STIMADOM Project)
(C. Salameh, C. Perchet, L. Garcia-Larrea)
• Coupling rTMS with immersive virtual reality
- Optimizing the effects of rTMS coupled with mirror therapy (STIRM Project)
(S. Grenouillet, J. Thomas, C. Quesada, R. Peyron)
- Cortical functional connectivity associated with treatment efficacy
(L. Malagutti-Modernell, C. Fauchon, I. Faillenot, R. Peyron)
• Cross-effect of rTMS in patients with pain and depression
Cortical stimulation target: primary motor cortex or dorsolateral prefrontal cortex (DoloDep Project)
(N. Oriol, S. Grenouillet, I. Faillenot, R. Peyron)
• Efficacy of rTMS of the motor cortex in neuropathic cancer pain (NeuroCanPain Project)
(S. Grenouillet, C. Fauchon, R. Peyron)
• Personalized transcranial electrical stimulation for pain relief (PersoStim Project)
(C. Salameh, N. André-Obadia, L. Garcia-Larrea)
• The contribution of dance therapy to adolescents (AlgoDanse Project)
(A. Bregeon, M. Frot, C. Perchet, G. Demarquay in collaboration with the
Pain Study Center of the Neurological Hospital)
-
Researchers
Philippe Convers
Jean Isnard
Amandine Rey
Michel Magnin
- Post-Doc or associate researchers
Juliette Gélébart (post-Doc, France)
Siloé Corvin (post-Doc, France)
Camille Fauchon (post-Doc, France)
Koichi Hagiwara (associated researcher, Japan)
Philip Jakson (Visiting Professor, Canada)
Benjamin Dominguez-Trejo (Visiting Professor, Mexico)
Emile Simon (associate researcher)
Agustina Lascano (visiting neurologist, Suisse)
Stéphanie Maza (associate researcher, France)
Fabio Godinho (Post-Doc, Brazil)
Nuuti Vartiainen (Post-Doc, FInland)
Florian Chouchou (Post-Doc, France)
Sigrid Shuh-Hoffer (Post-Doc, Germany)
Valery Legrain (Post-Doc, Belgium)
Ron Kuppers (Post-Doc, Belgium)
Blanca Diaz (Post-Doc, Spain)
Jordi Pedro (Post-Doc, Spain)
Lorena Guzman (Post-Doc, Venezuela)
Aline Acosta (Post-Doc, Brazil)
Cecilia Flores (Post-Doc, Spain)
- PhD
Emie Just (PhD, , Toulouse)
Hugo Barrillot (PhD, Ingénierie & santé, Saint-Etienne)
Louis Tremblais (PhD, Ingénierie & santé, Saint-Etienne)
Juliette Van Eycken (PhD, Neurosciences, Lyon)
Solène Grenouillet (PhD, Ingénierie & santé, Saint-Etienne)
Charbel Salameh (PhD, Neurosciences, Lyon)
Laura Malaguti-Modernell (PhD, Neurosciences, Lyon) 2025
Joy Thomas (PhD, Ingénierie & santé, Saint-Etienne) 2024
Siloé Corvin (PhD, Neurosciences, Lyon) 2023
Juliette Gélébart(PhD, Neurosciences, Lyon) 2022
Argitxu Caldichoury (PhD, Neurosciences, Lyon) 2022
Camille Fauchon (PhD, Ingénierie & santé, Saint-Etienne)
Charles Quesada (PhD, Ingénierie & santé, Saint-Etienne)
Benjamin Pommier (PhD, Ingénierie & santé, Saint-Etienne)
Christophe Nuti (PhD, Ingénierie & santé, Saint-Etienne)
Claire Bradley (PhD, Neurosciences, Lyon)
Claire Czelkala (PhD, Neurosciences, Lyon)
Lea Claude (PhD, Neurosciences, Lyon)
Anaïs Chapon (PhD, Neurosciences, Lyon)
Laure Mazolla (PhD, Ingénierie & santé, Saint-Etienne)
Florence Borgetto-Pomares (PhD, Neurosciences, Lyon)
Aurelia Poujois (PhD, Ingénierie & santé, Saint-Etienne)
Florian Chouchou (PhD, Neurosciences, Lyon)
Estelle Raffin (PhD)
Laure Peter-Derex (PhD, Neurosciences, Lyon)
Joseph Maraawi (PhD)
Mustafa Mahmutoglu (visiting PhD, Germany)
Marcos-Fortunato-de-Barrios Jr (visiting PhD, Germany)
Marina Pidal (visiting PhD, Spain)
German Prados (visiting PhD, Spain)
-
master out of Lyon or St-Etienne
Emie Just (Master, Toulouse)
Clementine Pouliot (Visiting Master, Canada)
Marie-Hélène Tessier (Visiting Master, Canada)
Nyamh Joyce (Master Erasmus, UK)
Ruth Kirby (Master Erasmus, UK)
Temitope Lana (Master Erasmus, UK)
Eva Masson (Master, Bordeaux)
Elisa Redavide (Master Erasmus, Italy)
Inès Jani (Master, Canada)
Martin-Schulz (Visiting Master, Germany)
Quentin Welniarz (Master, ENS Paris)
Isabelle Faillenot, webmaster de l'équipe NeuroPain